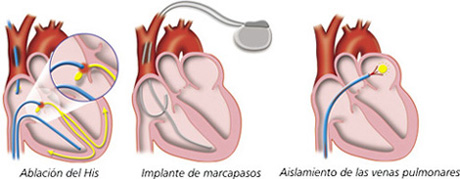
This is a technique for treating different types of tachycardia . Under local anesthesia, the cardiologist i ntroduce through a vein a flexible small tubes ( catheters) which are placed in the heart using x-ray images. Once in the heart the origin of the arrhythmia is located and at this point one of the catheters deliver heart or cold (crioablation) to ablate (destroy) the abnormal cardiac tissues that t are involved in the induction and/or maintenance of a cardiac arrhythmia.
2. Implantable cardioverter-defibrillator (ICD)
It is a small electronic device similar to pacemakers that is placed inside the left side of the chest to prevent sudden death from cardiac arrest due to life-threatening abnormally fast heart rhythms ( i.e. ventricular tachycardia or fibrillation ) or cardiac arrest. These devices are able to detect episodes of life-threatening arrhythmias, i.e. ventricular tachycardia or fibrillation. If this occurs, the DAI delivers immediately an electrical "shock(s)" to the heart to terminate the abnormal rhythm and return the heart rhythm to normal. Thus, the ICD rapidly defibrillate the heart of the patient. Many modern devices can distinguish between ventricular fibrillation , ventricular tachycardia , and more benign arrhythmias like supraventricular tachycardia and atrial fibrillation .
The ICD consist of a generator (which contains a battery and the circuit responsible for releasing electrical impulses and receive and interpret the patient's heart impulses ) and cables that conduct electrical impulses from the heart to the generator and vice versa. The battery, which lasts between 5-8 years, has a capacitor that stores energy to be downloaded to the heart.
The ICD also can sometimes act as a pacemaker in patients with a very slow rate of heart beat ( bradycardia). In addition , the ICD can store data on the patient's heart rhythm during hours that can then be evaluated by a cardiologist .
3. Electrical cardioversion
It is a medical procedure that applies an electrical discharge that produces the immediate conversion of any arrhythmia to the normal sinus rhythm . I t is indicated in the treatment of atrial fibrillation and ventricular arrhythmias such as ventricular tachycardia or ventricular fibrillation . To perform synchronized electrical cardioversion two electrode pads are placed on the chest of the patient, or one is placed on the chest and one on the back, which are connected to the defibrillator. The defibrillator paddles are placed on the chest and through it was a shock to the heart . The discharge stops all electrical activity of the heart and then allows normal heart rhythm returns . Sometimes it is necessary to apply multiple discharges to regain normal rhythm .
4. Pharmacological cardioversion
Following the intravenous administration of certain antiarrhythmic drugs it is possible to restore the sinus rhythm.
5. Cardiac pacemaker
It is an electronic device capable of generating electrical stimuli to regularly stimulate the heart . Each time the device delivers an electrical impulse , the heart contracts and pumps blood to the tissues . Pacemakers are of very small size , are placed ( implanted) under the skin , usually at the level of the clavicle and connected to the heart through an electrode. The implantation is relatively simple and is performed under local anesthesia . There are multiple types of pacemakers , and the indication of each one depends on the type of arrhythmia and the patient's condition . C urrent pacemakers have an average life of between 7 and 12 years; afterwards the battery should be replaced.
6. Antiarrhythmic drugs
They are a very heterogeneous group of substances that suppress/prevent heart rhythm disturbances. They are prescribed to the patient with three objectives: 1) to restore normal heart rhythm; 2) alleviate the patient's symptoms (palpitations, fatigue, syncope) and prevent complications (thromboembolism, heart failure), which can be achieved, both by removing or reducing the frequency of arrhythmia, for preventing recurrence or relapse , the arrhythmia, and 3) extend survival and reduce the risk of sudden death.
Antiarrhythmic drugs remain the treatment of choice for most patients with cardiac arrhythmias. However, they are difficult to handle because they are ineffective to control certain cardiac arrhythmias and can lead to significant adverse reactions, which limits their administration in some patients. Therefore, the prescription of antiarrhythmic drugs must always be under close medical supervision and initially should be prescribed by the cardiologist. Currently, antiarrhythmic drugs are, along with other non-pharmacological strategies (implantable c ardiac defibrillators, pacemakers, catheter ablation and surgery) the basis for the treatment of cardiac arrhythmias.
It is importatnt to remember that many patients undergoing catheter ablation or with implantable defibrillator carriers often require the administration of antiarrhythmic drugs to control recurrence of arrhythmias.